When EMTALA hits your ED, the response clock is measured in days, not weeks. We are building the tool you wish you had on day one.
The typical EMTALA path moves fast: surveyors are commonly onsite within roughly 2 business days of a complaint, the termination track runs about 23 days, and the Plan of Correction window is around 5 days for IJ-level findings. Clearpol's Plan of Correction Writer already drafts responses to federal and state survey deficiencies for hundreds of facilities. EMTALA support is in active development, designed by a former CMS Region 6 EMTALA physician reviewer. Same engine. Built for the way EMTALA actually works.

The stakes for your ED
EMTALA is the highest-stakes citation an emergency department can receive. And the only one where the clock runs against you while the decision is still being made.
EMTALA decisions don't end with the surveyor.
The State Survey Agency gathers the facts. The final EMTALA determination involves a CMS Regional Office medical officer, with peer-physician review through a QIO. Your Plan of Correction is part of what that physician reviewer reads before the tag is finalized.
That means your response is not a confession. It is a physician-review-ready defense. You need to argue the chart, the on-call list, the timeline, the policy, and the operational reality of your ED. Then layer the CMS-required corrective elements on top.
EMTALA doesn't follow the usual IDR-style path. Your Plan of Correction is what the reviewing physician reads.

The math is not subtle.
One prevented termination action, one downgraded CMP, or one PoC that does not get rejected for missing an element can pay for the subscription many times over.
Most EMTALA events trip three or four tags. At $136,886 per violation, a single ED incident can produce roughly $300K to $500K in modeled CMP exposure before DOJ involvement.
Average ED Director hours spent drafting a single EMTALA PoC manually, plus coordination across medical staff, compliance, and outside counsel. Five days, often including a weekend.
Typical retainer for outside counsel or a compliance consultancy to draft a single EMTALA PoC at $400 to $800 per hour. Sometimes higher when the response requires expert clinical review.
Even one prevented citation can pay for years of the subscription.
The product can save 30+ hours of director time, help narrow or remove tags before they become CMPs, and help prevent PoC rejection (which restarts the clock). For an active ED at a 100+ bed hospital, modeled annual EMTALA exposure can run in the high six figures. The subscription is a small fraction of that.
The same POC Writer your peers already trust. EMTALA-aware.
If you have seen Clearpol POC Writer in action for federal and state survey citations, the EMTALA module looks and feels the same. Upload your CMS-2567. Drop in your evidence. Get a structured first draft per cited tag, written for the physician reviewer and ready for your compliance leader to sign.
Upload the CMS-2567
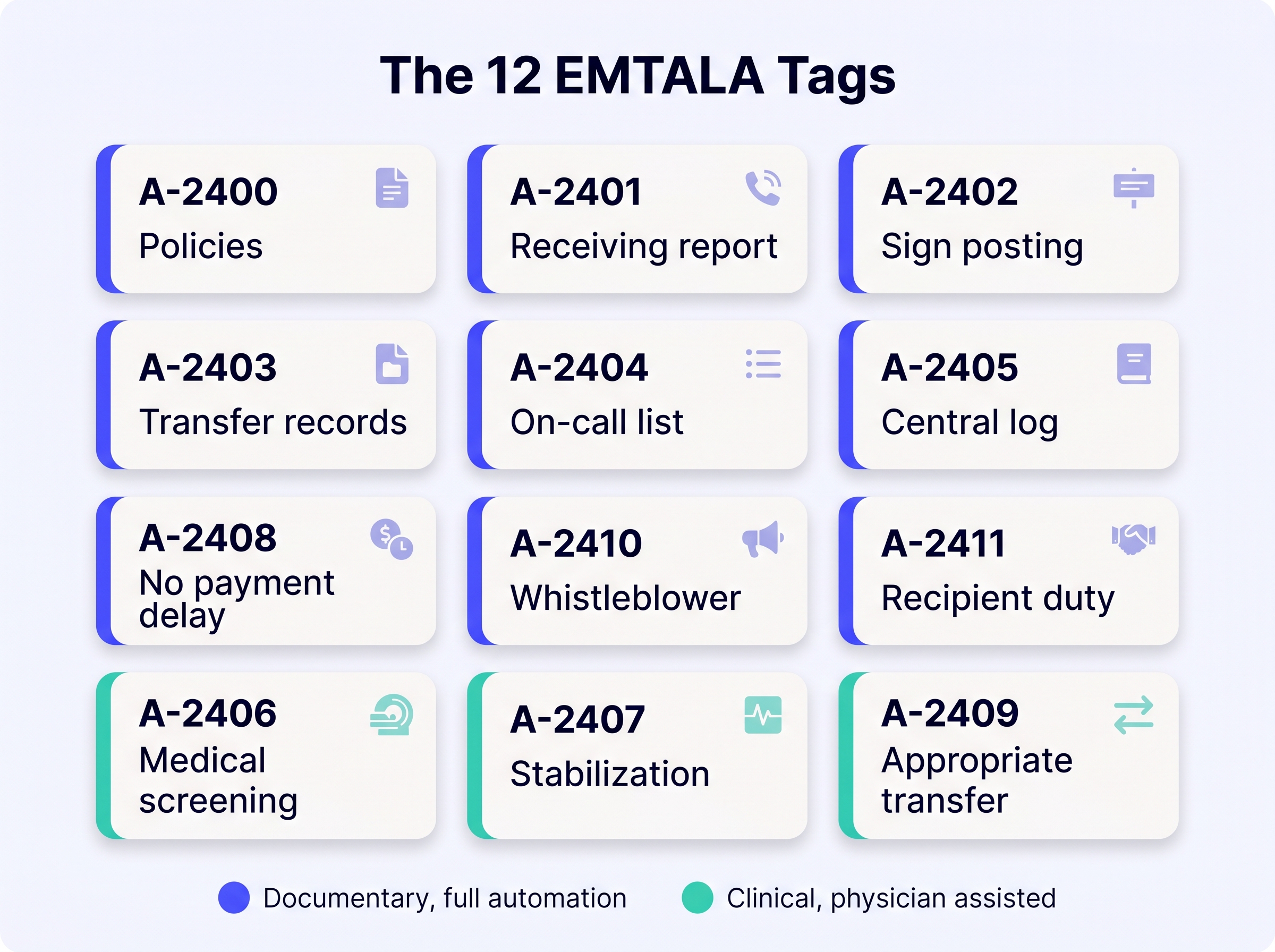
Drop in the Statement of Deficiencies. The system identifies each cited EMTALA tag (A-2400 through A-2411), pulls the regulation text, and maps the right defense pattern for each one.
Add the ED evidence
Upload chart pages, the ED central log, the on-call schedule, signage photos, transfer records, and your current EMTALA policy. The system pulls only what each tag needs. BAA-protected.
Review and export
First draft per tag: factual narrative, defense argument, and all CMS-required corrective elements. Compliance leadership reviews and signs. Export as a marked-up CMS-2567 ready for your State Agency.

Twelve tags, two defense modes, one workflow.
Most EMTALA citations are not just one tag. A single patient event commonly trips three or four. Each one needs a different evidence package and a different defense pattern.
Documentary tags (policy, signage, central log, on-call list, transfer records, payment delay, whistleblower, recipient duty) are drafted end-to-end by the system.
Clinical tags (medical screening, stabilization, appropriate transfer) are drafted from the chart with physician review. Every sentence ties back to a specific chart page, log entry, or policy paragraph. Auditable. Defensible. Fast.
The CMS-required POC structure.
Plans of Correction get rejected for missing one element more than for any other reason. Rejection restarts the clock. The system enforces the structure on every draft, every tag — and drafts export without patient or staff identifiers.
Corrective action
For the individuals affected by the deficient practice.
Look-back audit
Identification of other individuals with the potential to be affected.
Systemic change
Policy, training, or process change so the practice does not recur.
Monitoring plan
Measurable, with audit cadence, sample size, threshold, and escalation.
Implementation procedure
The step-by-step rollout that puts the systemic change into operational practice.
Completion date & responsible owner
A specific date and named responsible owner per cited deficiency, with IJ removal handled first.
"The surveyor is normally judge and jury. For an EMTALA, the surveyor is not the judge and jury. The surveyor literally just gathers the information."
Former CMS Region 6 EMTALA physician reviewer. Region 6 reviewed more EMTALA cases than any other region in the country.
Every defense pattern in the product is grounded in what the reviewing physician actually reads. The way the PoC is structured, the order of arguments, the citations to chart and policy, all of it reflects how the QIO and CMS Regional Office actually evaluate these cases.
Questions ED Directors ask us
When does EMTALA support actually launch?
In active development now. We are accepting a small number of early-access hospitals to pilot with. Book a demo and we will reach out as slots open. ED Directors at hospitals we have spoken to get priority.
Does this require Epic or any EHR integration?
No. Your team uploads the relevant chart pages, ED log, and supporting documents as files. We are not in the EHR. That keeps the integration footprint small and the security posture clean.
Is there a BAA?
Yes. A hospital-specific Business Associate Agreement is signed before any chart-touching workflow is enabled. Documentary tags (signage, policy, central log, on-call list) can be drafted without chart access at all.
What if our EMTALA classification is the new 45-day non-IJ category?
Same product, longer runway. Most EMTALA citations are still 5-day IJ, so the dashboard centers the IJ clock. Non-IJ cases get the full 45-day timeline without changing the workflow.
Does this handle the IDR?
EMTALA doesn't follow the usual IDR-style path. Disputes are typically worked out through the PoC response and the QIO physician review, which is exactly what this module is built for. For non-EMTALA hospital citations where IDR is available, ask us about the IDR add-on.
Who is the buyer inside the hospital?
Usually the ED Director, the VP Regulatory Compliance, or the Chief Medical Officer. The product is structured so the ED Director starts the response and the Regulatory Compliance Director signs and submits. Both reviewers see the same draft, comment on it, and approve without re-typing.
What does it cost?
Annual subscription per facility. Pricing is on the call so we can size it to your ED volume and EMTALA exposure. Most hospitals find it pays for itself with one prevented termination action or CMP.
See EMTALA POC Writer in action.
Book a 20-minute demo. We will walk your team through the EMTALA workflow, the tag-by-tag drafting engine, and the Plan of Correction structure built by a former CMS Region 6 EMTALA physician reviewer.
Book a demo